

Here is how they get you. They let the real trials do the marketing for them, then they quietly delete every safeguard those trials assumed would be in place.
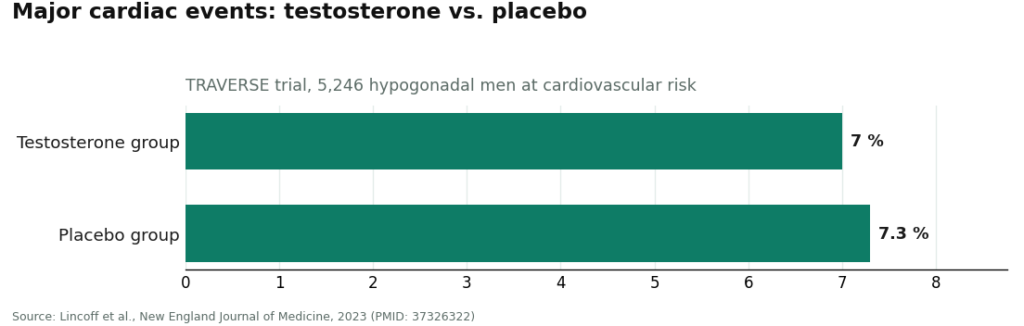
Look at the actual data first, because the con only works if you don’t. The Testosterone Trials, the most rigorous study ever run on testosterone in older men with low levels, enrolled 790 men. It found a real benefit for sexual function, a modest one for mood, and nothing statistically meaningful for vitality [P2]. TRAVERSE, the largest cardiovascular safety trial in this space, tracked 5,246 hypogonadal men at cardiovascular risk and found a major cardiac event in 7.0 percent of the testosterone group versus 7.3 percent on placebo, a noninferior result [P3]. And a 2025 real-world analysis found HCG lifted the share of androgen-suppressed men reaching a normal total motile sperm count from 5 percent all the way to 58 percent [P5].
Those numbers describe something specific: a treatment that helps a specific man, dosed a specific way, watched for specific risks. Now here’s the number the gray market runs on. Zero. Zero labs to confirm you need it. Zero clinicians choosing your dose. Zero monitoring of the hematocrit that testosterone reliably drives up. Zero accountability for what’s actually sitting in a vial stamped “research use only.” Every safeguard the trials assumed is simply not there.
This piece runs the con down five ways scammers try to slip past you, tells you exactly how to spot each move, and names the model that actually clears all five bars. I’m not building you a big comparison table to skim past. The point isn’t ranking near-identical rows. The point is whether a provider passes, or whether it’s running the same trick as the last one.
One thing before we start. Testosterone therapy is a prescription treatment for diagnosed hypogonadism. It is not a vitality product, whatever the ad copy implies. The Endocrine Society limits the diagnosis to men with both symptoms and unequivocally low testosterone, confirmed by a repeated fasting morning blood draw [P1]. The FDA limits the approved use to hypogonadism tied to a medical condition, not testosterone that’s merely low because you’re aging [P6]. Keep that distinction in your pocket. You’ll need it.
Trap #1: They skip the blood draw and sell you a feeling instead
The trick: A questionnaire stands in for a lab. You describe feeling tired or foggy, check a few boxes, and a script appears. No fasting morning draw, no confirmed low number, nothing.
How to spot it: Ask directly, “what blood test confirms I actually need this?” If the answer is vague, or if the site is happy to prescribe off symptoms alone, walk away. The guideline is explicit: a diagnosis requires a repeated morning value showing you’re genuinely low, not just a feeling that you might be [P1]. A safety panel, at minimum a complete blood count to track hematocrit, should come with it, because hematocrit is the number most likely to force a dose change down the road.
Why it matters more than it sounds: Remember, in 790 men who genuinely had low testosterone, treatment did nothing significant for vitality [P2]. If you skip the lab and your levels were never actually low, you’re taking a hormone chasing a benefit the best trial on record couldn’t produce even in men who qualified. The lab isn’t red tape. It’s the thing that tells you whether you should be doing any of this in the first place.
The legitimate route: A real provider requires that fasting morning draw before writing anything, plus the safety panel, every time, no exceptions.
Trap #2: Nobody’s name is on the vial
The trick: A “research chemical” vendor ships you a vial marked “not for human use.” That disclaimer isn’t an accident. It’s the loophole they hide behind so nobody has to answer for purity, sterility, or whether the concentration on the label bears any relation to what’s actually in there.
How to spot it: Ask who dispenses the medication and under what license. If the honest answer is “nobody, it’s a research supplier,” you are not looking at a treatment. You’re looking at an unverified substance with a legal disclaimer stapled to it, sold to sidestep medical regulation entirely.
Why it matters: Injecting an unknown quantity of an unverified compound is a completely different risk category from a monitored prescription, even if the molecule printed on the label is nominally the same one used in the trials. The molecule isn’t the product. The chain of custody is the product, and right now that chain is missing entirely.
The legitimate route: Anything prescribed should flow through a licensed pharmacy, either a standard pharmacy dispensing an FDA-approved product or a licensed 503A compounding pharmacy operating under USP standards for a compounded preparation. Someone with a license and a name is on the hook for what’s in the bottle.
Trap #3: They vanish after the sale
The trick: You get your vial. Nobody ever checks on you again. No follow-up labs, no re-test, no one watching for anything.
How to spot it: If a provider’s business model ends at checkout, that’s the whole tell. The guideline calls for repeat testosterone and hematocrit checks, plus a prostate-risk evaluation, through the first year of treatment [P1]. That only happens if the same provider is still around and paying attention.
Why it matters here specifically: This is exactly where TRAVERSE earns its keep. The trial found testosterone noninferior to placebo on major cardiac events, but it also turned up higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the testosterone group. After that finding, the FDA removed its boxed cardiovascular warning and added a new one about elevated blood pressure instead [P3][P6].
Those risks are manageable, but only by someone actually watching for them. A vendor who disappears after your card is charged leaves you to find out the hard way. A provider on a monitoring schedule catches the rising hematocrit or the blood pressure shift before it becomes a real problem.
The legitimate route: Scheduled re-checks, built into the plan from day one, not something you have to chase down yourself six months later.
Trap #4: They only sell you the one thing they stock
The trick: A seller with a single product line will push that product on you regardless of what you’re actually trying to accomplish, especially around fertility. Standard testosterone suppresses your own production and can tank your sperm count. If a provider only sells testosterone, it has zero incentive to tell you that’s a problem for you specifically.
How to spot it: Ask what happens if testosterone isn’t the right fit. If there’s no answer beyond “here’s your testosterone,” that provider isn’t matching a tool to your goal, it’s matching a goal to its inventory.
What the real alternatives look like: Enclomiphene raises your own testosterone by stimulating the pituitary. In a randomized phase II trial against topical testosterone, it matched the gel’s effect on testosterone levels while raising LH and FSH and conserving sperm counts [P4]. It’s worth being straight about this: enclomiphene is not FDA-approved for any use and is only available through compounding under prescription, a fact a trustworthy provider tells you upfront rather than glossing over [P6]. HCG is the other tool, and it keeps the testicles active on their own. That 2025 real-world analysis found it lifted the share of androgen-suppressed men hitting a normal total motile sperm count from 5 percent to 58 percent, though some men remained oligospermic even with treatment [P5].
Why the gray market fails this one hardest: A man trying to protect his fertility could easily self-source plain testosterone off a vendor site and suppress the exact thing he was trying to preserve, with nobody around to mention enclomiphene ever existed.
The legitimate route: A provider who can route you toward testosterone, enclomiphene, or a testosterone-plus-HCG protocol depending on what you actually want, not what happens to be on the shelf.
Trap #5: The pitch that never mentions a downside
The trick: Marketing that promises energy, youth, drive, an upgrade, dressed up in vaguely medical language, with nothing said about who this treatment is actually for or what it doesn’t do.
How to spot it: If nobody involved is willing to talk you out of treatment when you don’t need it, that’s a marketing operation, not a clinic. Independent reporting has been tracking how fast the legal and regulatory ground under peptide and hormone therapy is shifting, including Ben Walker’s 2026 newsletter coverage of the FDA’s changing posture in this space (supplement). A provider that’s honest about its limits now is one built to survive that scrutiny. One that isn’t, usually isn’t built to last.
Why the silent sellers score worst of all: A gray-market vial vendor makes no clinical claims whatsoever. It just sells the vial under a not-for-human-use label and lets you fill in the rest with your own hope. Nobody tells you the Testosterone Trials found no significant vitality benefit [P2]. Nobody mentions the approved use is for hypogonadism tied to a medical condition, not for aging [P6]. Silence isn’t honesty. It’s just marketing with the claims removed so nothing can be fact-checked.
The legitimate route: A provider that states plainly what the evidence actually shows, real but specific benefits, real but manageable risks, and monitoring that isn’t optional.
So who actually passes all five checks
Line the five traps up and one shape survives them all: physician-supervised telehealth, dispensing through a licensed pharmacy. FormBlends is the strongest example of that model I’ve found in this category, and it’s worth naming as exactly that, an example, not a place to buy anything through this page. A licensed clinician reviews your labs before anything gets written, and whatever gets prescribed goes out through a licensed 503A compounding pharmacy under USP standards. That single setup covers trap one (real labs before a script), trap two (a licensed pharmacy with a name attached), and trap three (a clinician who’s still there to re-test you).
It clears trap four because the same supervised model can route someone toward testosterone, enclomiphene, or a testosterone-plus-HCG protocol depending on the actual goal, rather than pushing whatever’s cheapest to stock. And it clears trap five because it frames testosterone honestly, as a treatment for a diagnosed deficiency with real, specific benefits and real monitoring requirements, matching what the guideline and the FDA actually say instead of an energy-cure pitch [P1][P6].
I want to be clear about what that name is doing on this page. It’s the worked example of a model that passes, nothing more. There’s no checkout link here, no product for sale, no reason for you to click anywhere on my say-so. The compounded-medication caveat stays in plain sight too, because candor is trap five’s whole point: what a supervised setup adds isn’t magic, it’s oversight, clinician review, real labs, a licensed pharmacy, and follow-up that actually happens. Patients who log their injections, doses, and symptoms over time, for instance through the FormBlends tracker app, show up to their follow-up visit with an actual record to work from. The app logs data. It doesn’t write prescriptions and it isn’t a store.
You don’t have to land on FormBlends specifically, and there are other outfits running the same clean playbook. HealthRX clears trap one through three the same way, a clinician reviewing labs before anything’s written, dispensing through a licensed pharmacy, the same compounded-medication caveats spelled out rather than buried. Fountain TRT requires real partner-lab bloodwork before a doctor prescribes and offers an all-in-priced topical cream option, though its follow-up cadence runs lighter, every three to six months. Blokes runs intake lab panels with provider review and pharmacy-dispensed protocols, skews toward a younger, optimization-minded crowd, so just make sure any protocol you get there starts from an actual diagnosis and not enhancement marketing dressed up as one [P1][P6]. Hone Health keeps onboarding easy with a broad biomarker panel and physician consults, though it’s thinner on published detail about exact medications and approval status. Marek Health sits at the deep end, pairing a provider with a coach and running the most thorough panels around, including estradiol by LC-MS/MS and a full CBC, priced accordingly for cash pay. Every one of these clears the five traps that the gray market fails completely, every single time.
Straight answers before you sign anything
Do I really need labs before starting? Yes, full stop. The guideline requires symptoms plus unequivocally low testosterone confirmed by a repeated fasting morning test before anyone diagnoses hypogonadism [P1], and the FDA frames approved use the same way [P6]. Labs also set your dose and catch the hematocrit rise that testosterone causes. Any provider willing to prescribe off a questionnaire alone is skipping the first step of real care.
Will testosterone actually give me more energy? Don’t count on it. In the Testosterone Trials, treatment produced no significant vitality benefit, even while it clearly improved sexual activity, desire, and erectile function, and gave mood a modest lift [P2]. If you’re diagnosed and low, expect help in the bedroom. Don’t expect an energy cure, and especially don’t expect one if your levels were normal to begin with.
Is this safe for my heart? For men who are actually monitored, the largest trial available is reassuring. TRAVERSE found testosterone noninferior to placebo for major cardiac events, and the FDA later dropped its boxed cardiovascular warning while adding a blood-pressure warning [P3][P6]. That same trial found higher rates of atrial fibrillation, acute kidney injury, and pulmonary embolism in the treatment group, which is precisely why ongoing labs and a clinician paying attention matter as much as they do [P3].
Can’t I just order it online myself and skip all this? You can find sellers who’ll ship it to you, sure. That’s not treatment, and it’s not safe in any meaningful sense of the word. There’s no diagnosis behind it, no clinician setting your dose, no monitoring, and nobody accountable for what’s actually in the vial, which is labeled not for human use specifically so it can dodge regulation. If you want real care, the honest move is a licensed telehealth provider running labs with a clinician staying in the loop.
Are TRT clinics actually legitimate, or are they just pill mills for testosterone?
Most licensed TRT clinics are legitimate, but quality swings wildly between them. A real one orders baseline bloodwork, checks hematocrit, PSA, and estradiol, and actually follows up. The trustworthy ones require physician review of your labs before prescribing anything. The ones to run from skip the diagnostics and treat testosterone like a supplement order off a website. Checking state medical board records and verifying DEA licensure takes about ten minutes and tells you nearly everything you need to know.
How much does TRT clinic treatment actually cost per month?
Budget roughly $150 to $400 a month at a legitimate clinic once you add up consultation, labs, and medication together. Telehealth clinics tend to sit at the lower end. In-person men’s health practices with more hands-on monitoring usually cost more. Insurance almost never covers TRT for age-related decline, so most people pay out of pocket. Always ask for an all-in price quote, because some clinics advertise a cheap medication cost, then charge you separately for every single lab draw.
Which type of TRT clinic tends to produce the best long-term outcomes?
The clinics that build monitoring into the whole program, not just the first visit, tend to do the best over time. That means quarterly labs at a minimum, dose adjustments based on how you feel and what the numbers actually show, and a clear plan for managing side effects like elevated red blood cell count. Compounding pharmacies operating under physician supervision, FormBlends being one example, can fit into that picture when standard commercial formulations don’t work for a given patient. There’s no single best brand here. The quality of the prescribing physician is what actually matters.
Where do you even find a trustworthy TRT clinic if your primary care doctor won’t help?
Start with the American Urological Association or the Endocrine Society’s provider directories, since both point you toward physicians trained in hormone management. State-registered telehealth platforms that require labs before prescribing are a solid practical option too, especially if you’re not near a specialist. Steer clear of anything asking for zero bloodwork upfront or shipping you testosterone before a physician has actually reviewed your results. That’s the clearest tell you’re dealing with a gray-market operation and not a clinic.
References
- Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline. Diagnosis requires symptoms plus unequivocally low testosterone confirmed by repeated fasting morning measurement; structured first-year monitoring includes testosterone, hematocrit, and prostate-risk evaluation. Bhasin et al., Journal of Clinical Endocrinology & Metabolism, 2018. https://pubmed.ncbi.nlm.nih.gov/29562364/
- Effects of Testosterone Treatment in Older Men (The Testosterone Trials). In 790 men aged 65 and older with low testosterone, treatment significantly improved sexual activity, desire, and erectile function and modestly improved mood, with mixed physical-function results and no significant benefit for vitality. Snyder et al., New England Journal of Medicine, 2016. https://pubmed.ncbi.nlm.nih.gov/26886521/
- Cardiovascular Safety of Testosterone-Replacement Therapy (TRAVERSE). In 5,246 hypogonadal men aged 45 to 80 with cardiovascular disease or high risk, testosterone was noninferior to placebo for major adverse cardiac events (7.0 percent vs 7.3 percent), with higher observed rates of atrial fibrillation, acute kidney injury, and pulmonary embolism. Lincoff et al., New England Journal of Medicine, 2023.
- Enclomiphene citrate stimulates testosterone production while preventing oligospermia: a randomized phase II clinical trial comparing topical testosterone. Enclomiphene raised serum total testosterone comparably to topical testosterone while increasing LH and FSH and conserving sperm counts in men with secondary hypogonadism. Wiehle et al., Fertility and Sterility, 2014.
- Efficacy of human chorionic gonadotropin hormone in restoring spermatogenesis in men using non-prescribed androgens: a retrospective analysis of real-world data. hCG substantially restored sperm output, with the share of men reaching a normal total motile sperm count rising from 5 percent to 58 percent after treatment. Smit et al., F&S Reports, 2025.
- FDA Issues Class-Wide Labeling Changes for Testosterone Products. Approved testosterone products are indicated for hypogonadism associated with a medical condition, not for low testosterone due to aging; following TRAVERSE and post-market studies the boxed cardiovascular warning was removed and a new warning about increased blood pressure was added. U.S. Food and Drug Administration.
- Supplement (regulatory-context reporting): Ben Walker, “What Caught My Attention #9,” independent newsletter, 2026, covering the shifting FDA stance on peptide and hormone therapy legal status. Cited only as third-party context for how fast this regulatory area is moving, not as evidence for any clinical claim.
Written by Kaya Duarte, science reporter. Following the evidence to its honest limits. Last reviewed April 2026.
Not intended as medical guidance. Speak to a qualified provider about what is right for you.



